As countries around the world look to follow Australia’s lead in restricting young people’s access to social media, a new report by the eSafety Commissioner might give them reason to pause, at least temporarily.
Australia’s online watchdog found more than 80% of kids were still using an age-restricted platform, such as Instagram, TikTok or Snapchat, three months after the trailblazing social media ban took effect.
The report is the first in a series the commissioner will publish as part of a two-year evaluation process. It contains several other key findings which confirm earlier evidence that the ban isn’t quite going to plan.
Reductions in social media use ‘limited in scale’
The commissioner’s report presents findings from 803 children (aged 10–15) and their parents, drawing on national baseline survey data from just before social media restrictions took effect in December 2025, and data collected from a three-month follow up from March to April 2026.
Its aim isn’t to assess the long-term effectiveness of the policy, but to examine whether anticipated early changes are happening.
While the number of children holding accounts dropped from roughly 52% to 42%, the emerging picture for ongoing use of social media is concerning. As the report says:
Our findings suggest that three months after the commencement of the age restrictions, reductions in children’s use of age-restricted platforms and account ownership have been limited in scale.
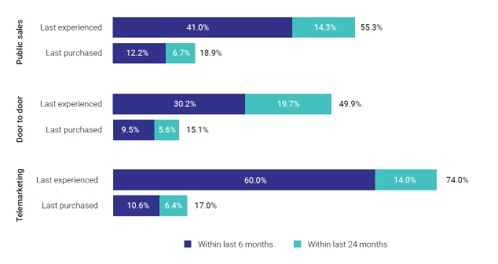
The “primary reason” for this was “ineffective implementation of age assurance measures by platforms”. In fact, more than half of kids surveyed said the platforms hadn’t even asked them to confirm their age. Some 18% reported platforms had incorrectly estimated their age to be above 16, and 37% said they had simply listed their age as 16 or above on their accounts to maintain access.
Prior to the restrictions being introduced, 85.9% of children reported using at least one social media platform. This number only dropped to 81.5% at three months.
“This may reflect the relatively low barrier to continued account access,” the report said, “with little need for children to rely on workarounds to obtain or maintain access”.
Alongside this, the report found “early signals” some children were moving to other platforms, such as Reddit and Pinterest. It also detected an “unintended consequence” of the ban: the proportion of parents who didn’t know their child had used social media increased by 10%.
And despite Prime Minister Anthony Albanese saying he hoped the ban would lead to more kids “playing outside with their friends”, the report found “little to no change” in what kids did offline three months after the ban took effect.
Unsurprising results
The results of this first evaluation are not surprising.
There have been regular media reports of children retaining accounts and getting around age-assurance checks.
And the findings reinforce the online regulator’s report from March, which raised concerns that social media platforms were not complying with the legislation.
The findings also echo other research showing children continue to access social media.
What happens next?
The report’s release is timely, given the government’s intention to “double down” on compliance by increasing penalties and expanding the commissioner’s information-gathering powers.
The government will now be under pressure to make good on its intentions to investigate non-compliance and, where appropriate, implement fines. The findings of this three-month report may bolster those investigations.
Earlier this week, the companies selling age-assurance software also called on the government to implement a “mandatory independent audit” of every platform covered by social media age restrictions, to test if they are using the tools properly.
The Age Verification Providers Association argues social media companies may opt to wear fines to see the legislation fail.
Yet even if companies comply and keep children under 16 from having accounts, this won’t stop kids accessing social media. The legislation does not restrict use in a logged-out state – and the three-month report shows children continue to access social media in this way.
All this should demonstrate to other countries that age-based restrictions are not a quick fix.
The government has committed to introducing digital duty of care legislation this year, which would hold technology companies to account and provide protections for Australians of all ages.
If we want to protect our kids from harmful content and algorithms on social media, that legislation cannot come soon enough.![]()
Lisa M. Given, Professor of Information Sciences & Director, Social Change Enabling Impact Platform, RMIT University
This article is republished from The Conversation under a Creative Commons license. Read the original article.






 The
The